In this course you will be taught how to critically interpret OCTs in ten patients who presented to our retinal service for assessment of diabetic retinopathy.
CASE
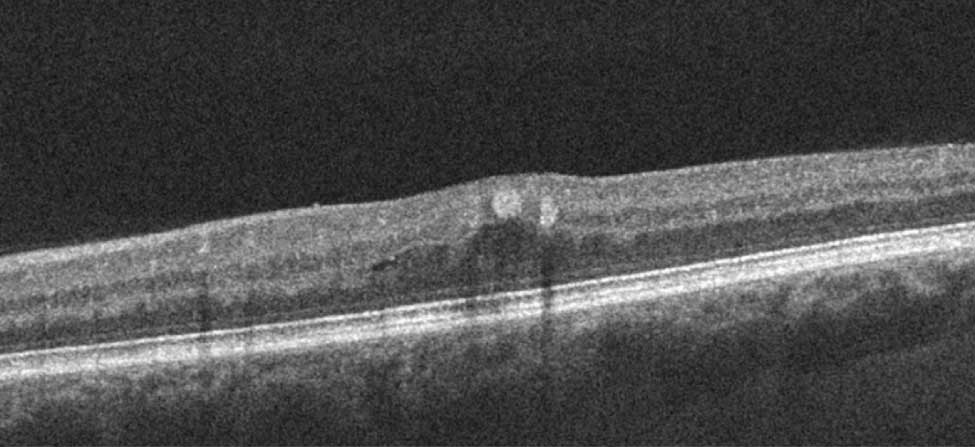
A 45-year-old woman presents with a 5-month history of blurred vision. You obtain an OCT.
What abnormalities are noted on the OCT?
The presence of an epiretinal membrane
Presence of an epiretinal membrane. An epiretinal membrane can be seen with diabetic retinopathy. If located, it is seen on the surface of the retina. It may or may not be associated with retinal distortion and macular hole formation.
Hyperreflectivity consistent with exudate
Correct
Hyperreflectivity consistent with exudation. Exudate which is due to lipoprotenacous material depositing in the retina is very hyperreflective and may be associated with deeper retinal shadowing.
Vitreous hyperreflectivity consistent with vitreous hemorrhage
Vitreous hyperreflectivity can be seen in patients with significant vitreous hemorrhage. This not seen here as the vitreous is optically clear.
Poor vision as the ellipsoid layer is absent
Poor vision as the ellipsoid is absent. The integrity of the ellipsoid layer and other retinal layers is correlated with visual acuity. Here, however, the ellipsoid is intact throughout the OCT image.
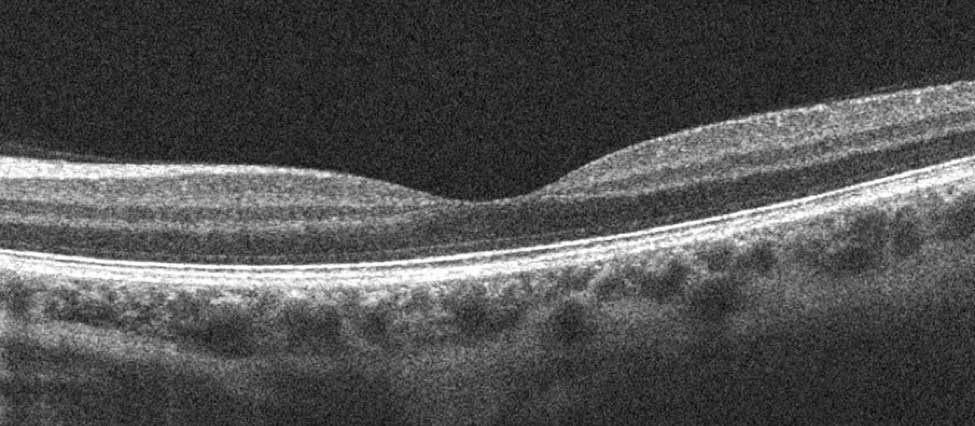
Introduction
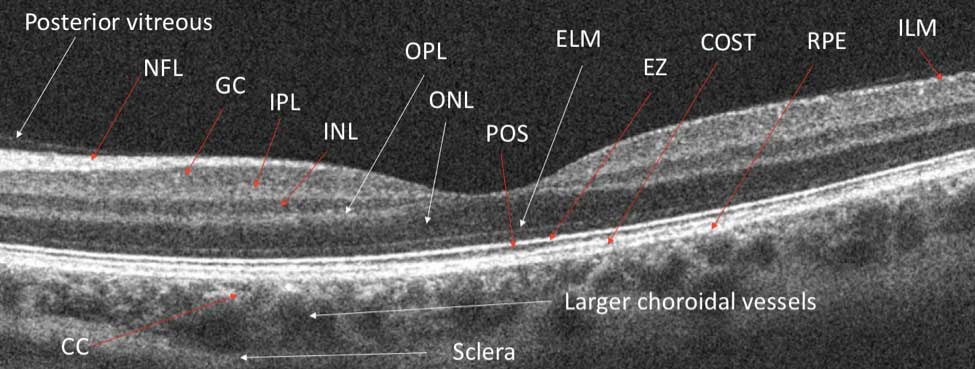
Before we review this and the other remaining cases, let us review a normal OCT. In the image below, can you identify the following layers:
posterior vitreous face,nerve fiber layer (NFL)
ganglion cell layer (GC)
inner plexiform layer (IPL)
inner nuclear layer (INL)
outer plexiform layer (OPL)
external limiting membrane (ELM)
ellipsoidzone (EZ)
cone outer segment terminal line (COST)
retinal pigment epithelium (RPE)
choriocapillaris (CC)
larger chrodoidal vessels and the sclera
This labeled diagram shows the important retinal layers. Here are some important points to remember:
The posterior vitreous may or may not be visible; if it is detached it may be visible. It may be partially or fully detached. The vitreous may also be more opaque in the setting of a vitreous hemorrhage.
The internal limiting membrane (ILM) is a thin hyperreflective line located at the anterior retina.
The nerve fiber layer (NFL) is a hyperreflective, relatively thick layer located just below the ILM. It gets progressively thicker the as the ganglion cell axons make a right angle turn to exit the eye through the optic nerve (here to the left of the image).
The ganglion cell layer (GC) is a darker layer that lies immediately below the NFL.
The inner plexiform layer (IPL) is a hyperreflective layer that separates the darker (hyporeflective) inner nuclear layer (INL) the GC layer.
The outer plexiform layer (OPL) is a hyperreflective layer separating the inner nuclear from the outer nuclear layer (ONL).
The outer nuclear layer (ONL) is a very thick and hyporeflective layer.
The external limiting membrane (ELM) is a thin hyperreflective layer.
The ellipsoid zone (EZ) – and formerly referred to as the inner/outer segment (IS/OS) junction appears as a thicker white line.
The thin line deep to the EZ is the COST line and represents the cone outer segment terminals. The dark line between the EZ and COST represents the photoreceptor outer segments (POS).
Deep to the COST is the retinal pigment epithelium (RPE). Bruch's membrane may or may not be visible deep to the RPE.
The choriocapillaris (CC) is seen as a vascularity in the inner choroid and the larger choroidal vessels as hyporeflective.
The sclera appears as a hyperreflective line posterior to the choroid.
When a patient with diabetic retinopathy is being assessed it is very important to thoroughly assess the “outer triple lines” — those being the ELM, EZ and COST lines, as there is a strong correlation between the integrity of these lines and visual prognosis.
Access Full Case Content
Get full access to the content of this case. Purchase this case now for $39.
Plus, save when you buy 3 cases.