A 64-year-old male is referred to your office on an urgent basis by their family doctor for a possible retinal detachment. On history, the patient complains of awakening with a “film” over his inferior visual field of the right eye. He has complained of occasional photopsia but no floaters. The patient's past ocular history is unremarkable. Past medical history is significant for hypercholesterolemia and well-controlled hypertension.
On exam, best-corrected visual acuity is 20/25 OD vs. 20/20 OS. There is no relative afferent pupillary defect and IOPs are within normal limits. The patient can count fingers in all 4 quadrants with both eyes.
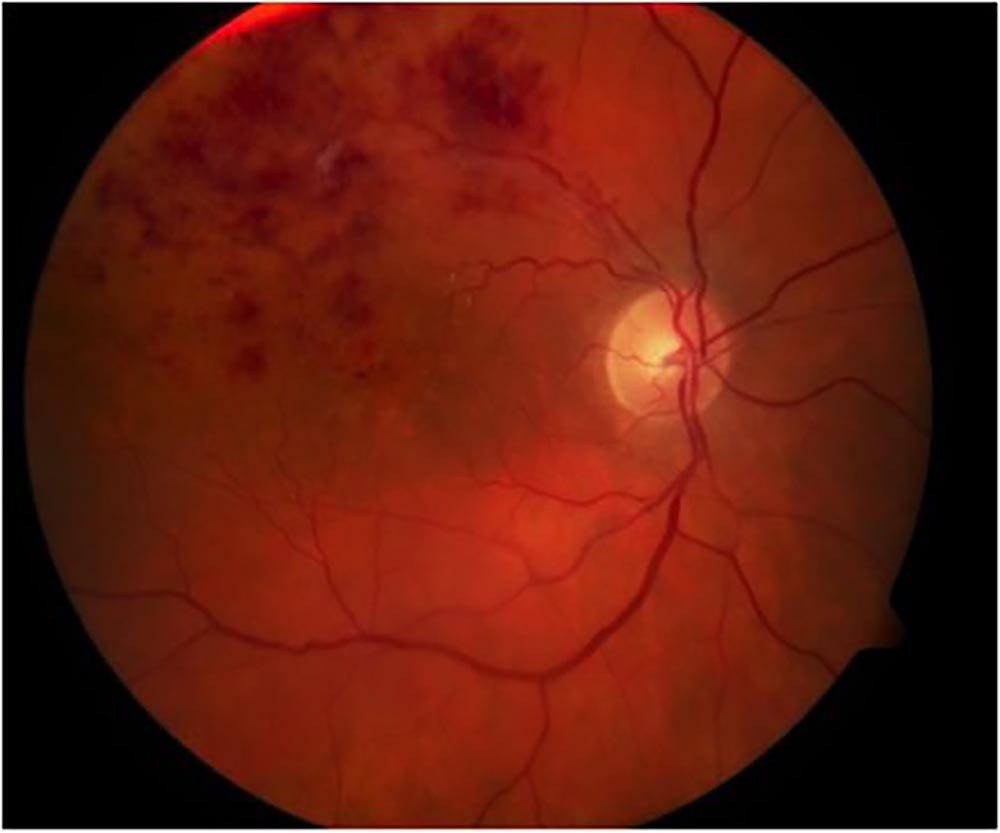
Anterior segment exam is unremarkable. Posterior segment exam of the right eye is shown below: